Hair thinning in women is common, distressing, and often misunderstood. The medical term for this condition is Androgenetic Alopecia, an umbrella diagnosis that includes both male and female pattern hair loss. When it occurs in women, it is called Female Pattern Hair Loss (FPHL).
Unlike Male Pattern Baldness, which typically causes a receding hairline and bald spot at the crown, FPHL presents differently — and the hormonal science behind it is more complex.
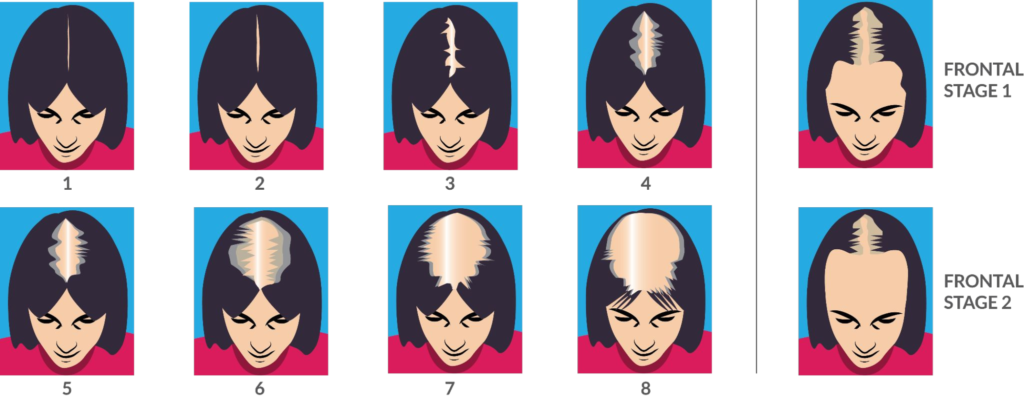
What Does Female Pattern Hair Loss Look Like?
An 8-Level Vertex and 2-Level Frontal Recession Scale — A Simplified, Clinically Practical Savin Modification for Female Pattern Hair Loss