Hyperpigmentation Disorders — Understanding Melasma and other causes of Uneven Skin Tone
Hyperpigmentation Disorders
Pigmentary disorders are very common skin concerns that can affect both appearance and overall quality of life. In some cases, they may also provide clues to underlying health conditions. Below are some of the more common conditions that we take care of at our office.

Melasma: How Pigment Forms in the Skin
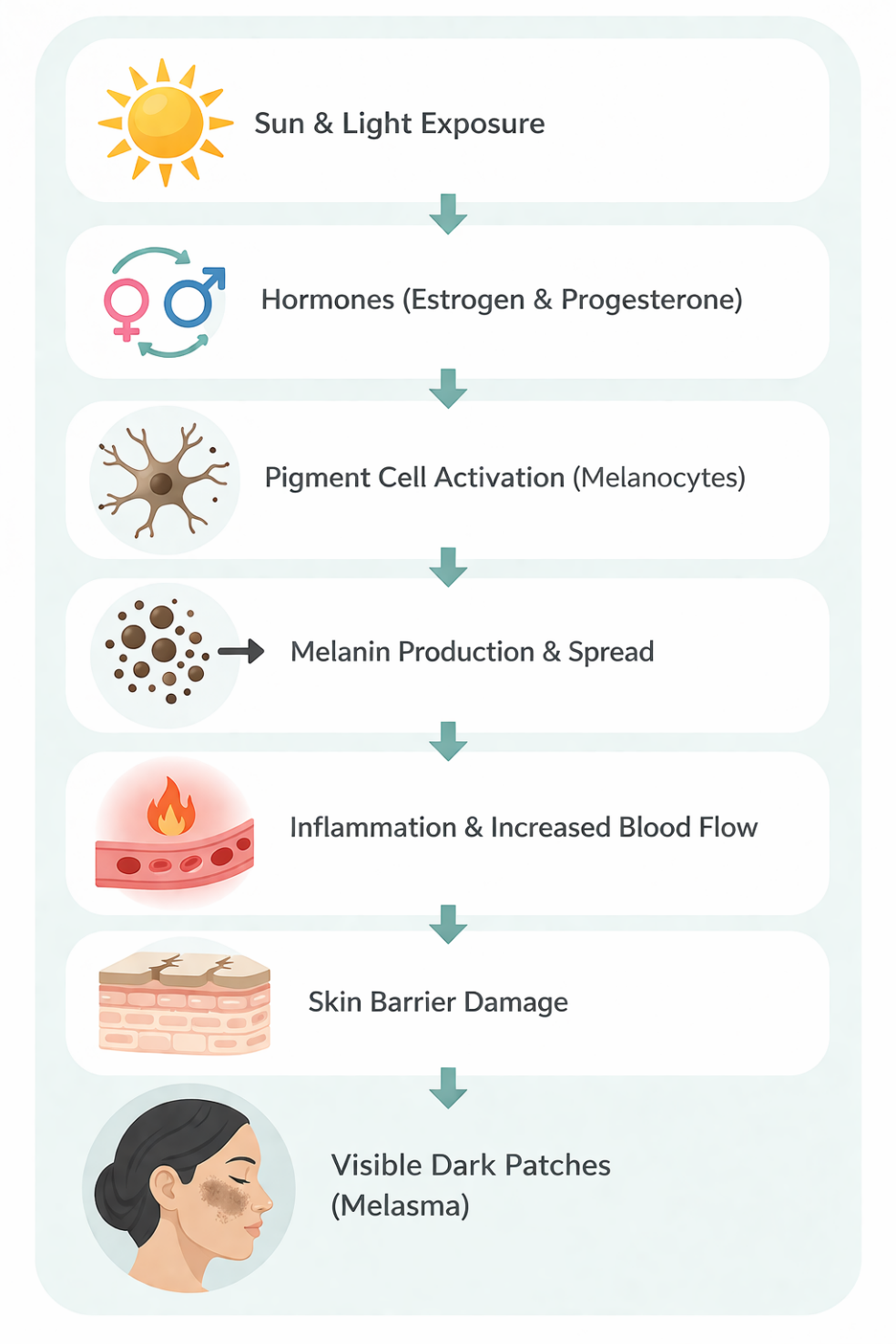
Melasma occurs when multiple factors work together to increase pigment in the skin. Sun and visible light trigger pigment production and oxidative stress, while hormones like estrogen and progesterone make pigment cells more sensitive and active.
These cells produce excess melanin, which spreads into surrounding skin and appears as dark patches. Inflammation and increased blood flow can make pigmentation worse and longer-lasting, and a weakened skin barrier makes the skin more reactive to triggers. Overall, melasma is caused by sun exposure, hormones, inflammation, and skin sensitivity working together.
Heat can worsen melasma even without sun exposure by triggering inflammation and activating pigment cells. It increases signals in the skin—like VEGF and prostaglandins—that boost melanin production, and activates the TRPV1 (heat) receptor, which also drives pigmentation.
Repeated heat exposure, such as from cooking or hot environments, can keep this process going. Heat also works together with visible and infrared light to further increase pigmentation.
Melasma: How Pigment Forms in the Skin
Melasma occurs when multiple factors work together to increase pigment in the skin. Sun and visible light trigger pigment production and oxidative stress, while hormones like estrogen and progesterone make pigment cells more sensitive and active.
Call Us
(720) 818-0533
These cells produce excess melanin, which spreads into surrounding skin and appears as dark patches. Inflammation and increased blood flow can make pigmentation worse and longer-lasting, and a weakened skin barrier makes the skin more reactive to triggers. Overall, melasma is caused by sun exposure, hormones, inflammation, and skin sensitivity working together.
Heat can worsen melasma even without sun exposure by triggering inflammation and activating pigment cells. It increases signals in the skin—like VEGF and prostaglandins—that boost melanin production, and activates the TRPV1 (heat) receptor, which also drives pigmentation.
Repeated heat exposure, such as from cooking or hot environments, can keep this process going. Heat also works together with visible and infrared light to further increase pigmentation.




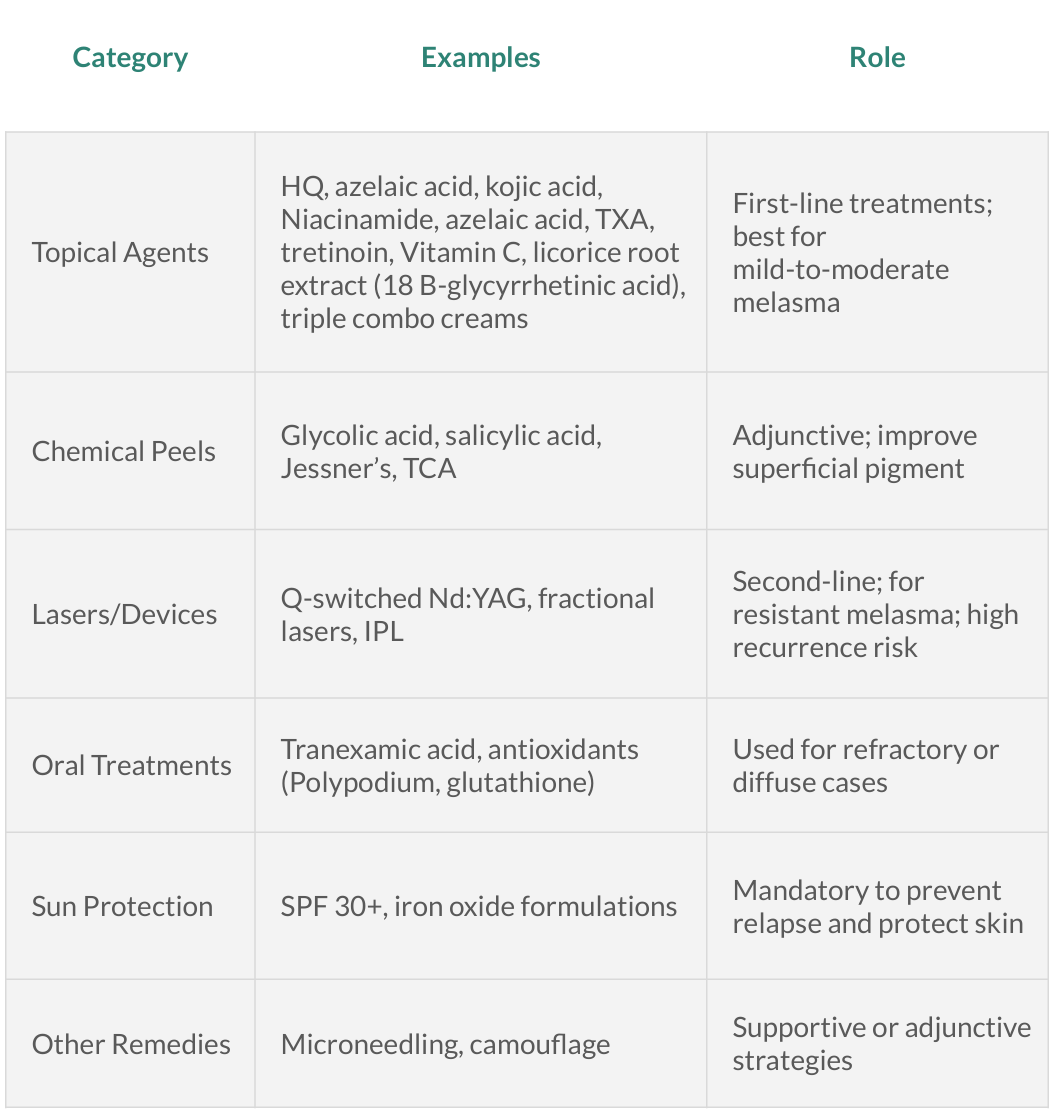
Treatment Options For Melasma
Topical Treatments For Melasma

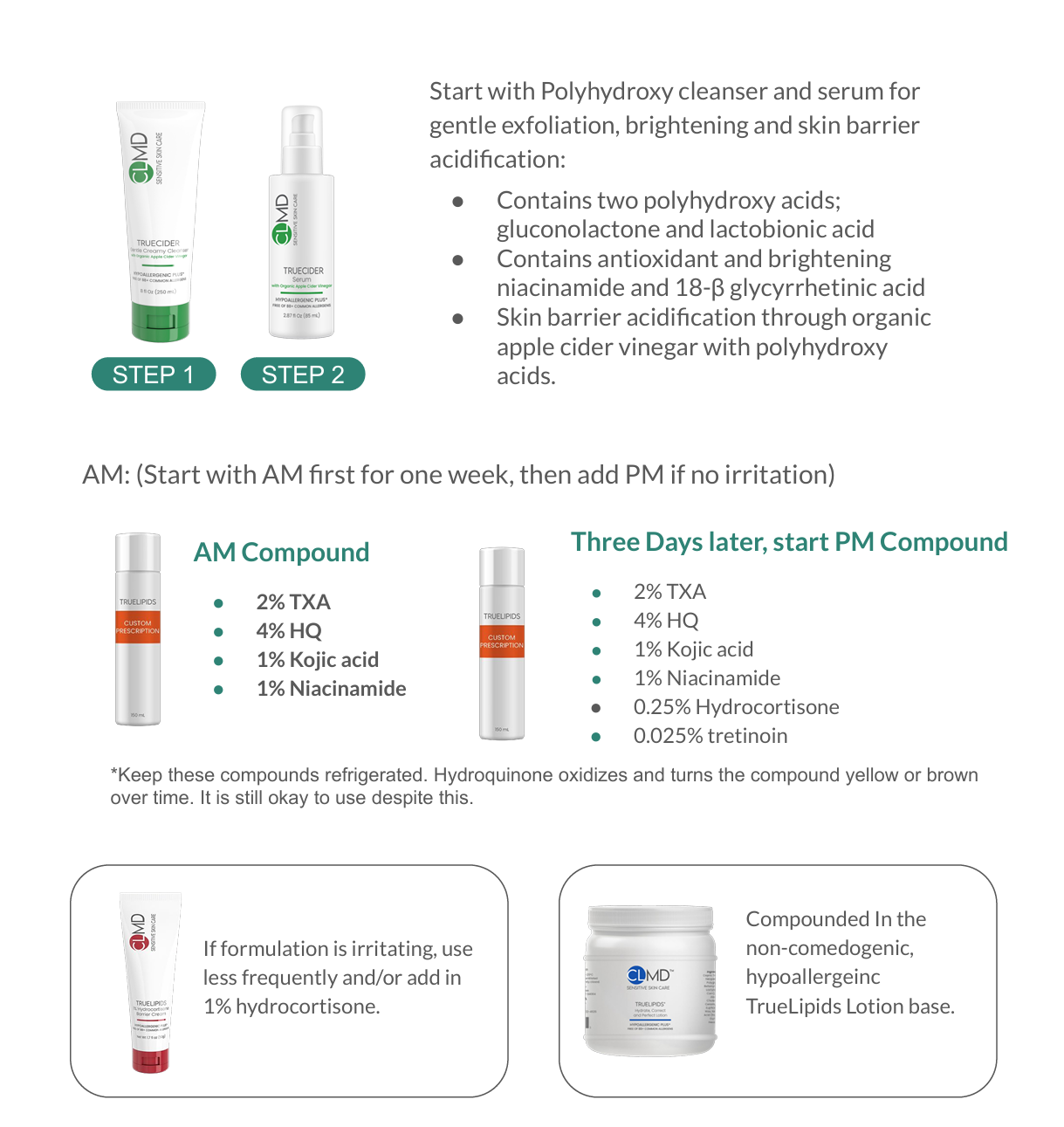
Our Clmd Melasma Treatment Protocol
Best Sunscreens for Melasma and Post Inflammatory Hyperpigmentation: Dermatologist-Recommended Protection for Clearer Skin
Chemical UV filters (e.g., oxybenzone, octinoxate, homosalate, octocrylene, avobenzone) are more likely to cause sensitization and photoallergic reactions, while mineral sunscreens with zinc oxide and titanium dioxide are generally non-sensitizing and better for sensitive skin. Iron oxides in tinted sunscreens provide added protection against visible light (especially blue light, 400–500 nm), which can worsen melasma and post-inflammatory hyperpigmentation, making them especially beneficial for pigment-prone patients.
Spironolactone is an oral anti-androgen medication used for blood pressure but also effective in dermatology for hormonal acne and melasma, especially in women. It works by blocking androgen (testosterone) receptors in the skin, reducing hormonal stimulation that can increase oil production and pigment activity. This helps improve melasma in patients where hormones are a contributing factor.
Ephelids (Freckles)
Ephelides, commonly known as freckles, are small, light-brown macules that typically appear in childhood and become more noticeable with sun exposure. They are most often found on sun-exposed areas such as the face and shoulders. Histologically, freckles are characterized by a normal number of melanocytes but increased melanin production, which explains their darker appearance without an actual increase in pigment cells. They tend to fade during the winter months or with consistent sun protection. Ephelides are more commonly seen in individuals with fair skin types (Fitzpatrick I–II) and are often associated with variants in the MC1R gene.

Ephelides, commonly known as freckles, are small, light-brown macules that typically appear in childhood and become more noticeable with sun exposure. They are most often found on sun-exposed areas such as the face and shoulders. Histologically, freckles are characterized by a normal number of melanocytes but increased melanin production, which explains their darker appearance without an actual increase in pigment cells. They tend to fade during the winter months or with consistent sun protection. Ephelides are more commonly seen in individuals with fair skin types (Fitzpatrick I–II) and are often associated with variants in the MC1R gene.
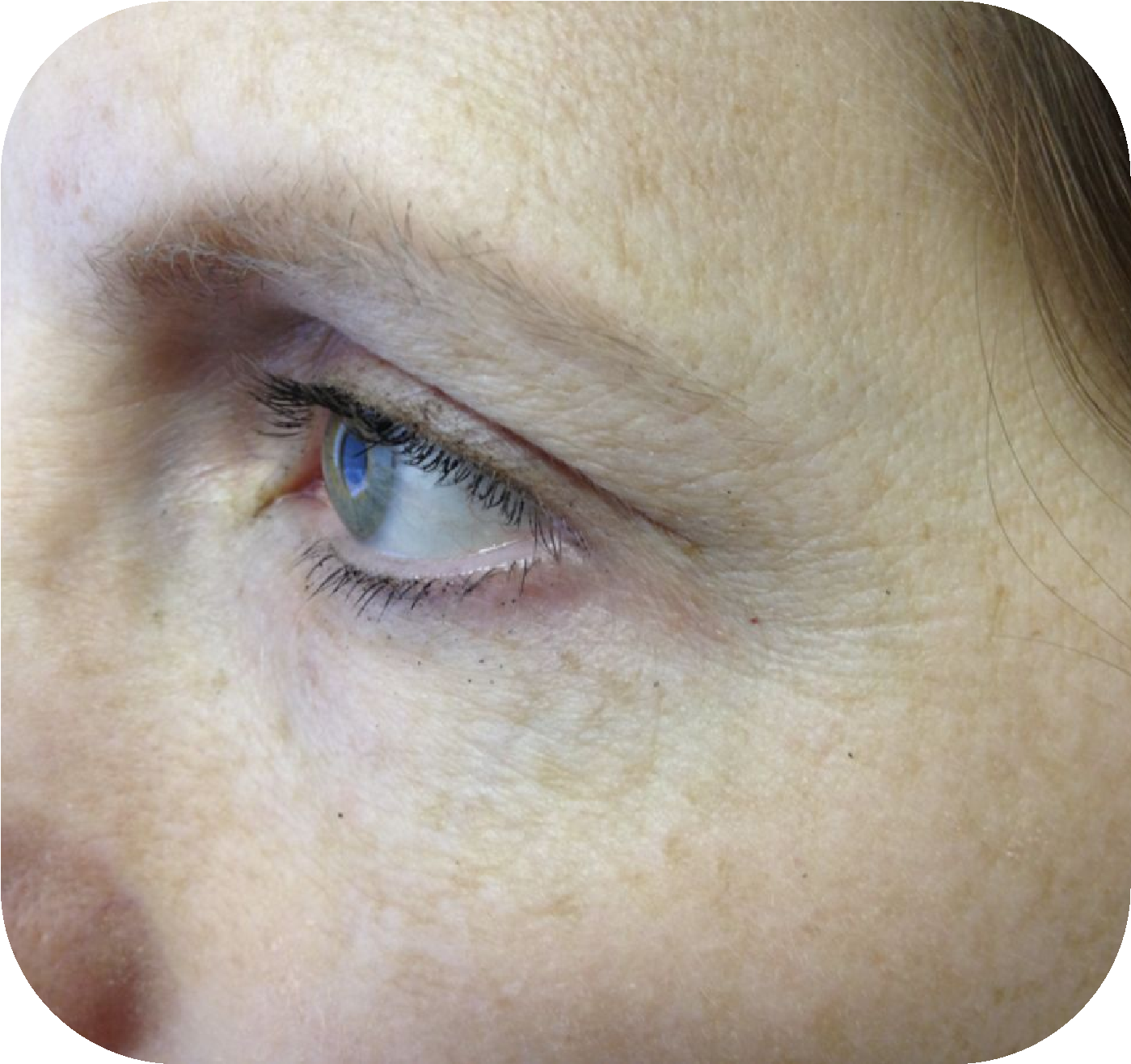
Solar Lentigo (Sunspots and Age-spots)
Solar lentigo (often called an “age spot” or “sun spot”) is a harmless dark spot caused by long-term sun exposure—not liver disease. It commonly appears on sun-exposed areas like the face, hands, chest, and shoulders, especially in fair-skinned adults. These spots are flat, well-defined, and range from light to dark brown. They develop over time as UV exposure increases pigment in the skin. While benign, they can sometimes resemble other skin conditions, so evaluation is important if they change. Treatment is optional and cosmetic, including topical lightening creams, chemical peels, laser therapy, or cryotherapy. Daily sunscreen is the best way to prevent new spots.


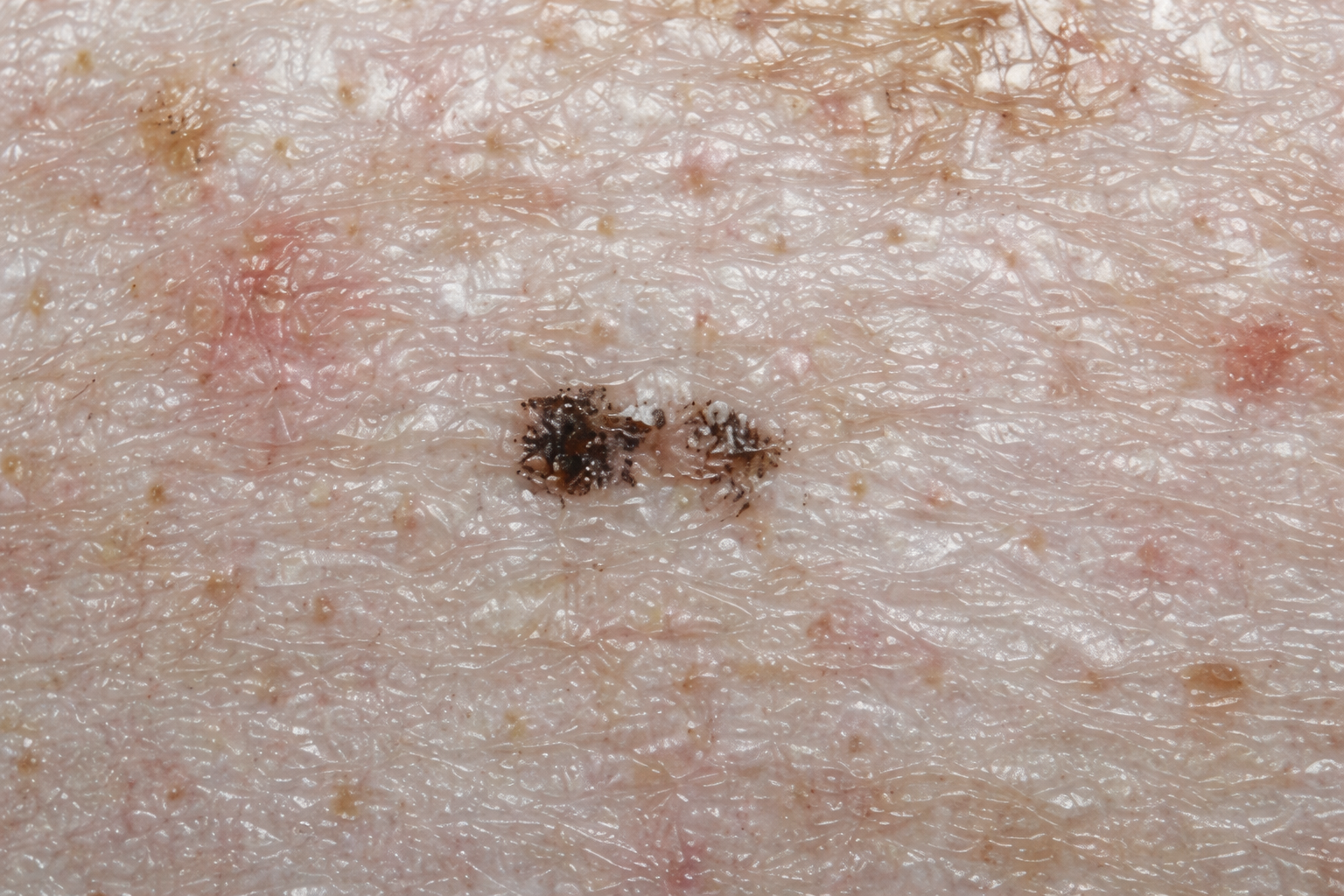
Ink Spot Lentigo (Ink Spot Sun Spot)
Ink spot lentigo is a harmless, dark spot on the skin that looks like a small drop or splash of ink. It’s a type of sun spot caused by long-term sun exposure and is most often seen in fair-skinned individuals.
These spots are usually small (often just a few millimeters), flat, and dark brown to black with irregular, jagged edges. They commonly appear on sun-exposed areas like the shoulders and upper back and typically don’t cause any symptoms.
Ink spot lentigines are benign and not cancerous, but because they can sometimes look similar to more serious skin lesions, it’s important to have any new or changing dark spot evaluated by a provider.
Treatment is not necessary unless for cosmetic reasons. Options may include laser treatments, chemical peels, or topical lightening products. The best prevention is daily sunscreen use and sun protection to reduce further skin damage.
Lentigo Simplex
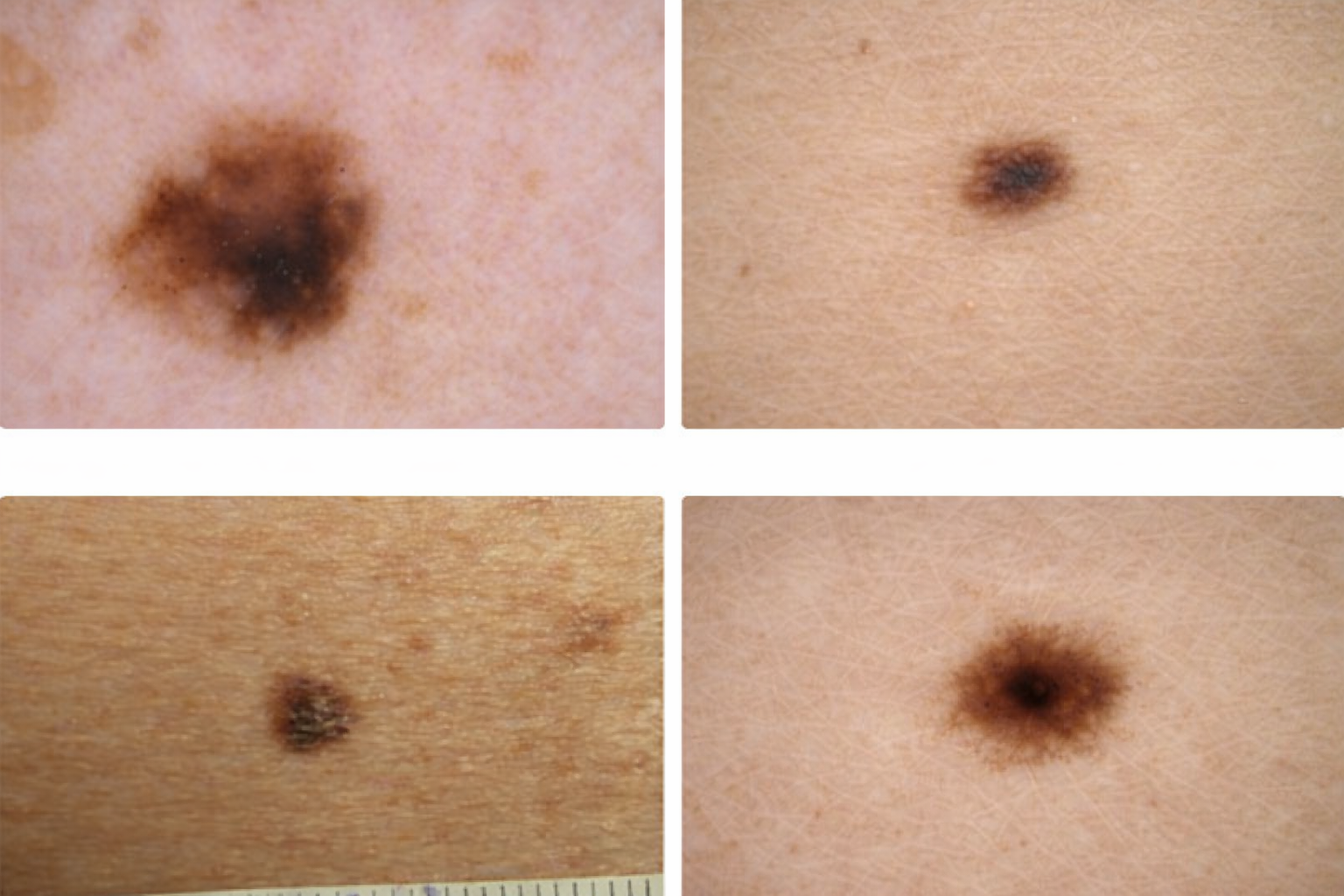
Lentigo simplex is a flat, persistent dark spot that is not caused by sun exposure. Unlike freckles, it can appear on sun-protected areas and does not fade with less sun. It may be present at birth or develop in childhood, but it can appear at any age. These spots are usually single, well-defined, and darker than freckles.
Under the microscope, lentigo simplex is a benign lesion with an increased number of pigment cells (melanocytes) in the lower layer of the skin, sometimes with mild structural changes. Because it can sometimes resemble more serious spots like melanoma, a biopsy may be done if the lesion is new, changing, irregular, or looks different from your other spots.
If you notice a dark spot that is growing, changing color, has irregular borders, bleeds, or looks unusual, it’s important to have it evaluated by your doctor.
Post Inflammatory Hyperpigmentation (PIH)
Post-inflammatory hyperpigmentation (PIH) is temporary skin darkening that appears after irritation or injury. It shows up as flat spots that can be brown, black, red, or purple, depending on your skin tone. PIH is not a scar, but it can take weeks to months—sometimes longer—to fade.


What causes it?
PIH develops when the skin produces excess pigment in response to inflammation. Common triggers include acne (the most frequent cause), eczema, psoriasis, insect bites, cuts or burns, cosmetic procedures (like peels, lasers, or microneedling), allergic reactions, and picking or scratching the skin. Inflammation overstimulates pigment-producing cells (melanocytes), leading to uneven pigment in the skin.
Post-Inflammatory Hyperpigmentation: Who Gets It & How to Prevent It
PIH can appear anywhere on the body but is most common on the face, neck, chest, back, and areas exposed to irritation or injury. Anyone can develop PIH, but it is more common and longer-lasting in individuals with darker skin tones or those with ongoing skin conditions like acne or eczema, frequent irritation, or picking at the skin.
Prevention focuses on simple steps: daily sunscreen use (preferably zinc-based), avoiding picking or trauma, using gentle skincare, and treating inflammation early. For patients prone to pigmentation—especially before procedures like lasers or peels—dermatologists often recommend short-term use of pigment-control ingredients such as tranexamic acid, hydroquinone, retinoids, niacinamide, or kojic acid to reduce the risk of PIH and promote more even results.
Treatment of Post-Inflammatory Hyperpigmentation (PIH)
PIH can be treated with a combination of topical skincare and, in some cases, procedures. Treatment focuses on reducing pigment and speeding up skin renewal.
Topical Treatments (First line)
Melanin-inhibiting agents:
Some forms respond to medical-grade skincare, while others require chemical peels, lasers, or light-based treatments. Without determining depth, treatment may be ineffective or even worsen pigmentation.
- Hydroquinone (2–4%) – gold standard (prescription or OTC in some countries)
- Azelaic acid
- Kojic acid
- Tranexamic acid
- Licorice root extract (18-β glycyrrhetinic acid)
Retinoids: Tretinoin or adapalene promote cell turnover. Vitamin C: Antioxidant and pigment-lightening. Niacinamide: Anti-inflammatory and inhibits pigment transfer.
Procedural treatments:
- Chemical peels (e.g., glycolic acid, salicylic acid)
- Microneedling
- Laser treatments (low energy, suitable lasers for dark skin only)
“Does Post-Inflammatory Hyperpigmentation Go Away?” Yes, post-inflammatory hyperpigmentation (PIH) can go away—especially superficial (epidermal) pigment, which often fades on its own within 3–6 months even without treatment, while deeper pigmentation requires treatment, takes longer and may never fully resolve.
Schedule Your Dermatology Consultation
Take the next step toward healthier skin.
Aesthetics & Medical Lasers of Colorado – Clinical Dermatology
Locations
700 Tenacity Drive #102 Longmont, Colorado, 80504
2801 Remington Street Suite 2, Fort. Collins, Colorado, 80525
Contact
720-818-0533
Office Hours
Monday-Friday 8:00 AM to 6:00 PM Saturday 10 AM to 2 PM Sunday: By Appoinment only
Aesthetics & Medical Lasers Dermatology
Get a Dermatology consultation and customized skin care solutions
Services
Work Hours
- Monday-Friday 8:00 AM to 6:00 PM Saturday 10 AM to 2 PM Sunday: By Appoinment only
- 720-818-0533
- 700 Tenacity Drive #102 Longmont, Colorado, 80504
- 2801 Remington Street Suite 2, Fort. Collins, Colorado, 80525
- Copyrigt © 2026 Aesthetics & Medical Lasers Dermatology
- Terms of Use
- Privacy Policy